Beloved
I don’t think I can bear this
It’s a good plan
To work five more years
And retire in better financial shape
House paid off
But it hurts so
My tattered bruised and battered heart
Already patched so many times
And to see so many people each day
Hurting
Why, Beloved?
Why don’t we mature?
Maybe I’ll be a tree again
Living wood
That bends and moves with the wind
That eats the sunlight
Drinks the rain
Endures the snow and drinks it as it melts
Until spring comes
And I stir and start to bud
Deciding when it’s time
To uncurl leaves in warm sun
_______________________
For the Ragtag Daily Prompt illusion. Or should it be delusion? Or survival? Or beyond that to peace?
Should we worry about bird flu? Oh, yes, I think so. I have been wondering why we still have chicken to eat and chicken in the stores, if millions of chickens are being wiped out to try to prevent H5N1 bird influenza from moving into humans. This article explains in unreassuring detail how factory farms, packing chickens together, and killing them at 6 weeks old for meat, puts pressure on the virus to become more deadly and kill the host. In wild birds the influenza virus wants to spread, so it’s better not to kill the host fast. That is not true on our national and international big factory farms.
Firing the people working the track the H5N1 bird influenza and trying to stop it if it starts going human to human, well. Is that injustice or arrogance or stupidity? Or all three? And who wants to work for the government now? It is being treated as a corporation, but it isn’t a corporation. Public service often pays less. Good luck hiring the best and brightest who want to serve our country and humanity.
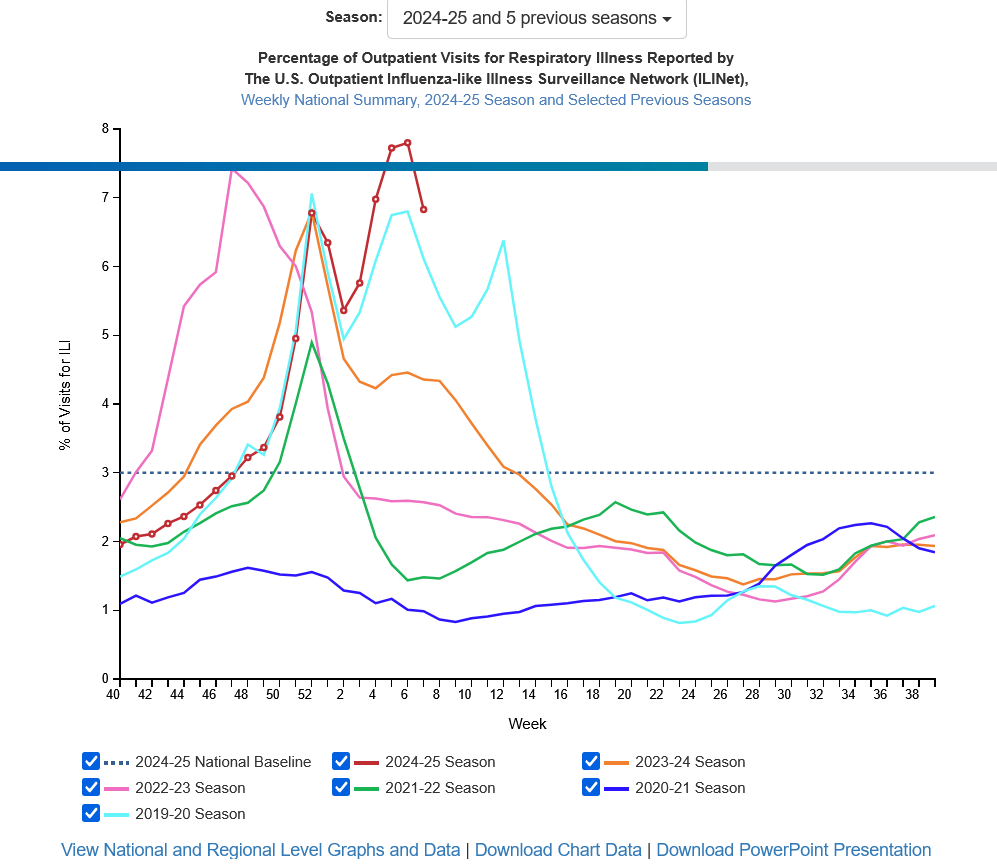
This is the worst year in the US for influenza since 2017-2018 so far. That is without the H5N1 bird influenza really getting in to people. Here is the graph for the week ending February 15th from the CDC. I keep an eye on it all through influenza season.
The article on H5N1 bird influenza is the best argument I’ve ever read for choosing not to eat meat. I like meat, but the factory farming is going to more countries. It may produce more eggs and more chickens, but if it is also the perfect breeding ground for lethal influenza, that changes my viewpoint. We cannot go on. We will have another pandemic.
I ran my own small clinic from 2010 to 2022, working somewhere else, got Covid, was on oxygen for a year and a half, did some healing and then came back to work.
There has been a culture change in medicine that feels very strange to me. I did not notice it because I was in a solo clinic and not “part of the system”.
All the doctors, providers, are more isolated. I got a compliment yesterday when I was doing a “warm hand off” of the most sick or complicated patients, three new diabetics, a person with cancer, a person with a genetic heart problem. The doctor who I was handing off to is in the same clinic but we have barely talked since May. I don’t know her at all. She complimented me on excellent care “and calling specialists”.
I thought, huh. But I think that is a dinosaur doctor thing. I think mostly people communicate through the electronic medical record email, send messages about patients. For the decade that I was solo, I had to call other specialists because I was on a different electronic medical record. The email didn’t connect. The hospital reluctantly gave me a “link” to their system, but it was only a link to look. I could not write or send anything.
About two months ago I got an echocardiogram result. I read it and thought, ok, it’s not normal but what does it mean? Outflow obstruction by the thickened heart wall. Hmm. I called cardiology and spoke to the cardiologist who read it. He sounded surprised and said, “Idiopathic hypertrophic cardiomyopathy, most likely. It’s a classic echo.” “So, what do I do?” “Send him to me.” “Anything that I should change meanwhile?” “Yes,” says the cardiologist. He had me stop one medicine and start another. “No vasodilators and the beta blocker slowing the heart rate should help decrease the outflow obstruction.” “Got it.” I said. He also gave me two more tests to order.
I referred the patient to cardiology but it was a month before he got in. The two tests were done and they ordered more. If the diagnosis is correct, he’ll be sent to a special clinic in Denver. I called my patient while we were waiting for the cardiology visit. The medicine change had not made much difference as far as he could tell.
I was also told when I got here that I would never get a local nephrologist to see a patient, they were two busy. However, I have called two nephrologists about two patients and both took the patient and again, gave me instructions.
Two specialties have been very difficult to contact: orthopedics and gastroenterology. I have no idea why they are so difficult.
I can see that email feels faster. But there is no human contact, asking follow up questions is difficult, I don’t get that bit of further helpful education: this is what you do next. I have learned so much over the years by touching base with specialists. Once I fussed at a patient to go to hematology oncology about their high platelet count. The patient didn’t want to. He came back and said, “Apparently I have this newly found genetic problem. They put me on two medicines, not expensive. And I feel better than I have in 20 years.” I asked the oncologist about it the next time I called. He lit up, excited, and told me about the JAK-2 mutation. It is so exciting to learn about new areas in medicine and my patient says, “I have to thank you for pushing me to see the oncologist. I feel so much better.” Wow and cool.
Clinic feels like I am mostly isolated, a silo, an island, rarely talk to the other physicians unless I go to find them. I think hospital administrations like this, keeping the physicians in line by having their schedule be so packed that they almost never talk to each other. What a good way to keep physicians from interfering in the money making production! Ugh, I think it is quite horrible and unhealthy for the providers and for our countries medical system in the long run. I was seriously less lonely in a solo clinic.
The prognosis for our current medical system is very poor. The patients say to me, “Why do my doctors keep leaving?” They aren’t attached, they are isolated, I don’t think the physicians know what they are missing. Colleagues. Not silos.
Honey is older, nearly thirty years since that first feeling of being bitten by ants. She is back in corporate medicine, as a temp. Temporary, short term, maybe that will work better.
It is a joy to go in a room and be alone with a person and their monsters. Theirs and hers. Sometimes the younger ones haven’t experienced it, they are terrified if one of their monsters becomes a little bit visible, they hate seeing them. Honey tries to be gentle. If they only want to talk about the sore shoulder and not the stress and violence, well, she leaves the door open a crack. Sometimes the monsters cry.
Older people may be stiff to start with, but when they realize their monsters are seen, acknowledged, this isn’t another robot doctor in to say increase your diabetes medicine, lower your diabetes medicine, tell them a plan without ever connecting, the older ones lean back, sigh, and relax. The monsters play on the floor, Honey’s monsters playing with theirs, happy, engaged.
The hard part is the clinic staff. Honey is with them daily. The medical assistants are young. They kick their monsters aside as they walk down the hall. It is terribly hard and heartbreaking to work at her desk, with the medical assistants’ monsters cowering under their desks, kicked, abused, silent tears and holding bruises. Honey’s monsters mind. They climb into her lap and hide their faces in her shirt, under her jacket, peer over her shoulder. They don’t understand! Why can’t she be nice to THESE monsters?
Honey whispers to her monsters when the medical assistants are rooming patients. “I am so sorry, loves. If I acknowledge these, the monsters of the women working, I become a demon. It is very hard to share an office, no wonder I worked in a clinic alone for eleven years.” Honey has been through that. It is still inconceivable that some people don’t see the monsters at all. Is it learned blindness? Or just not developed unless someone had to learn it? Unless someone grows up in terror and seeing the monsters is the only way to survive.
Honey thinks some people learn to see them as adults, at least their own monsters. Hard enough to do that, without seeing the monsters clinging to other people.
Honey is tired of her monsters crying in sympathy with the staff’s monsters. She thinks maybe there are small crumbs that she can leave for these demons. Little gifts. Her monsters can creep under the desk when she is the only one in the room and leave something. A flower. A dust bunny. A crumb of a crisp. A small rock. A little gift to let them know they are seen and loved. A poem. A prayer. Just a tiny bit of love.
Lily’s person moved two days ago, much closer. Supposedly to a place where Lily the cat can go, but instead of a private room, there is a roommate. It took me a month to get Lily cat to let me pat her, so the roommate won’t work. We are all very very frustrated. And next week daily treatments for Lily’s person start, thirty minutes away, without enough warning to get volunteer drivers. So it will be me. I am tired. But I suppose it’s anti-matter, right? We were given 24 hours notice by the nursing home and by the physicians about both the move and the treatment and they wanted to start the treatment the same day that she was moving. Whether we can provide all the transport seems to be irrelevant.
The stealthie is from Whidby Island. Right, I’m just an irrelevant shadow as far as the medical dysfunctional machine is concerned.
The United States could go to single payer healthcare, but one objection has been “People will lose their jobs with health insurance companies.” Yet no one seems to object to AI, Artificial Intelligence taking jobs. It’s technology so it’s fine! The wave of the future! Coming whether we like it or not!
One form of single payer healthcare is medicare for all. Expand medicare so that it covers everyone. At first, it only covered retired female teachers. Women were only considered for teaching jobs if they were single. A married woman was expected to work in the home. The teaching pay was low. Men were expected to be supporting a family, so they got more. Women were often supporting parents or children if spouses died or divorced or abandoned a family or were disabled. Early census information was a finagle: any male in the household was listed as “head” even if it was an elderly disabled father or a boarder or a teen. So the true numbers of women as head of households were obscured.
Single payer would improve healthcare. There would be ONE set of rules. Physicians would know if something was covered. Right now there are over 500 health insurance companies and they each have multiple different policies. Not only that, but the policies can change monthly in what they cover. Did you know that? I would get monthly postcards from multiple companies saying that I could go on line to one of the 500 different websites and see what they had changed and were no longer covering. I found little time to learn 500 websites. We spend enormous amounts of healthcare money on communication back and forth from insurance companies to hospitals and clinics. Trying to prior authorize CT scans, MRIs, surgeries, referrals, medications (even old cheap ones!) and then attempting to get the health insurance companies to pay for the care. Remember that the insurance companies are allowed a 20% profit: so for 1 million dollars of healthcare money, $200,000 can go to profit. The people and computer work is not in that profit, so what percentage of your healthcare dollar goes to attempting to prior authorize and get paid? How much of your healthcare dollar would you like to go to healthcare?
Medicare’s overhead is either 1.4% or 6%, instead of that 20% profit and the prior auth/collection effort. There are two different estimates (from here):
1. There are two different measures of Medicare’s administrative costs. One figure comes from the Medicare Board of Trustees’ annual report, while the other comes from CMS’ National Health Expenditure Accounts. According to the latest trustees’ report, Medicare’s overhead represented 1.4 percent of its total expenditures. According to the latest NHEA, Medicare’s overheard was 6 percent of expenditures.
2. The discrepancy between the two figures is due to Medicare Parts C and D. Mr. Sullivan wrote that the difference between the trustees’ measure of overhead and the NHEA measure “is due almost entirely to the fact” that the NHEA figure includes administrative expenses incurred by health insurers that participate in Medicare Advantage (Part C) and Medicare’s prescription drug program (Part D). In essence, the overhead associated with the private insurers involved with Medicare raise the program’s overhead by almost 5 percent, or $24 billion in 2010.
People worry about “socialized medicine” but really, the closest system to socialized medicine is the Veterans Administration. I don’t think anyone wants to take their healthcare away, and some of it is specialized depending on where they were deployed and what they were exposed to. I saw veterans in my clinic because we were more than 30 miles by car from a VA hospital.
What about medicare fraud? I saw way more fraud with the insurance companies. Companies will maximize revenue by sending equipment at the exact interval insurance allows (like sleep apnea equipment and diabetes glucometers). It doesn’t matter to them if it’s being used or not. After my father died, there were 16 full oxygen tanks full in his house. The company was happy to pick them up and no, they did not want to reimburse the payments. A biller told me that often the health insurance companies will pay less then the contracted amount. When challenged, they say, “Oh, that was a computer error! We will fix that!” She said, “I have never once seen the error in the physician’s favor.” When I had cobra insurance, they would not pay my bills and I had to call them every single time to force them to pay. It took enormous amounts of time and again they claimed, “Oh, computer error!” I finally called their counseling line and said, “I want to be counseled for your company refusing to call me back and screwing over this cobra policy, and by the way, I have a family member dying of cancer.” That finally made them fix it.
WHY is our culture ok with technology taking jobs, while improving healthcare can’t? Get rid of the health insurance companies! Medicare for all! If we all had secure health insurance, think of the work innovation in our country!
Today’s Ragtag Daily Prompt is anachronism. I guess that would be Helen Burling Ottaway’s watercolors, since an AI can do them, and my work as a physician. The American Academy of Family Practice (AAFP) wrote: “So, the AAFP looked into an AI assistant for clinical review that can “pull the data together in a problem-oriented manner and give you a snapshot of exactly what’s going on with your patient without having to search and click and find things.”
Um. Ok, I am thinking of a patient who was about to be transferred from our small hospital to a bigger one. His notes came across my desk. I called the hospitalist. No less then four physicians during the hospitalization, starting with the emergency room physician, had written that his abdomen was “flat, soft, non-tender, no masses”. What this told me was that 1. Not one of them had done an exam. 2. Not one of them had read my notes nor the surgeon’s notes. 3. The bigger hospital was going to laugh themselves silly if they did an exam. Why? He had an 8 by 8 inch enormous umbilical hernia present for 20+ years, which had not gotten fixed yet because of other medical issues.
Great. So let’s make it worse by having an AI pick out what is important from the patient record and have it make up exams, which people are too lazy to do. Physicians are too lazy to do. People, you had better read every single note your doctor or nurse practitioner or physician’s assistant writes, because you want to go on record in writing when they get it wrong. It is an absolute horror show. Read your notes, because your doctor is most likely not reading the notes from the specialists. I find it amazing, horrifying and sloppy.
I learned to paint watercolors from my mother. I am not primarily an artist, but I learned all sorts of techniques from her. We do not learn from plugging an idea into a computer. We learn from doing. And yes, it is work to learn techniques, but it is worth it!
I was pricing health insurance in case I get well enough to work more. I can get an $800 a month with a $8000 deductible or a $1435 a month with a $2000 deductible. I would very much like to work part time treating Long Covid. But, ironically enough, looks like I can’t afford health insurance. It costs more than the malpractice would. Ironic, huh? It’s not like we need doctors. (I do not have a medical release yet anyhow, but time to do research. It’s making me gloomy.)
You know, if we do get Artificial Intelligence, it will take one look at the United States Medical non-system, decide we are insane, and wipe us out.
And honestly, when I was working for the hospital clinics, I thought the most brilliant person in our office was the woman who could extract a prior authorization from so many insurance companies. I would send the referral to print and half the time she would have it authorized by the time the patient got to the front desk. And why do we waste all that brilliance on giving health insurance companies a profit of 20 cents out of every dollar? That is $20,000,000 out of $100,000,000. Looks worse with bigger numbers, doesn’t it?
I did a porch call a bit over a year ago. It’s like a house call except on a porch.
A friend/patient asks me to see a long time friend of his. The friend has multiple chemical sensitivities. We meet, the three of us, on his porch.
My friend has had me as a physician but he has not seen me at work with someone else.
I ask a lot of questions and then launch into an explanation of the immune system and how antibodies work.
My friend states, “He can’t understand that.’
I smile at his friend. “Oh yes he can. And you followed what I said, didn’t you?”
His friend grins back and said, “Yes, I did. Most of it. Or enough.”
All of my patients are smart. One day in clinic I think how blessed I am, that ALL of my patients are smart and fascinating people. Then I think, how could that be? And, how lucky am I?
And then I think: everyone is smart.
They are not all educated in the same way I am. They may not be well read. They may not have my science background or my geeky fiction and poetry and song brain. But they ALL are smart.
Some are brilliant at mechanical things. I have a patient who is an expert in restoring church organs and is working 3000 miles away in New York City. “They are driving me crazy.” he says. “You have to have the approval signed off on over 20 groups, historic preservation, the fire fighters, etc, etc, to remove one board from the church. The organ was covered over by bad repairs over the years. We’re trying to get it back. After this I will put in new organs, but this is my last restoration.”
Veterans, teachers, attorneys, physicians, retired computer engineers, car mechanics, marine engineers, parents, grandparents. They are all smart, men and women.
We finish the porch visit with some options and the friend of my friend says he will think about what I said and try some things.
A few days later my friend calls. “I couldn’t believe he was following your science talk, but he was. He got it. He remembers it and understood it.”
“Of course he did,” I say.
“I am actually impressed,” says my friend. “It was really interesting watching you do that.”
That may be one of my weird skills. To be able to listen to the person thoroughly and then respond in language that they understand and a bit more. An assumption, always, that they can follow a complex and intricate idea.
I do not know if they always follow what I say. But they always respond to the assumption that they are smart and that they can understand and that they are an equal. I am explaining from my expertise, but I know they can understand when I explain it correctly.
And I have not seen this in the physicians that I have seen. Out of 22 physicians since 2012, four were excellent and met me and explained as an equal.
The rest did not. They dismiss me. They talk down or avoid me once they realize that they do not understand why I keep getting pneumonia. They are afraid to say “I don’t know.” Four are not afraid and recognize that it’s something weird and say, “We do not understand this and we don’t know how to fix it.”
Four out of 22 have my respect. And that is a sad number. Medical training needs to change and physicians need time to listen and need to learn how to listen.
Meanwhile, all of my patients are smart. And I am so blessed.
I had cobra from my job in 2009 and the insurance company refused my bills. Not one bill. Not once. EVERY BILL EVERY TIME: 1. my healthcare 2. my son’s healthcare 3. my daughter’s healthcare 4. my daughter’s orthodontia 5. my dentist 6. my son’s dentist. I had to call EVERY TIME to get them to pay. Calling an insurance company takes 25 or 30 minutes, right? Eventually I asked for customer service who first said it was my fault because “you probably paid the bill late”. I said, “No, I was on time every month.” Then customer service wouldn’t call me back. I finally called their COUNSELING HOTLINE, since it said I would be “paid” $30 to get counseled, and said, “MY LITTLE SISTER IS DYING OF BREAST CANCER AND THE THING THAT IS MOST STRESSING ME OUT IS YOUR INSURANCE COMPANY WON’T PAY THE COBRA BILLS AND I HAVE CALLED CUSTOMER SERVICE OVER AND OVER AND THEY WON’T CALL ME BACK. HOW ABOUT YOU COUNSEL ME HOW TO DEAL WITH THAT!” And I cried. I got a call back from the head of customer service saying “Oh, it’s a computer glitch and we had you misfiled. We have fixed it.” They “misfile” people all the time, or drop patients if they get sick, or say the person didn’t pay on time. I HATE INSURANCE COMPANIES. Anyhow, be warned that insurance companies are there to earn money and will try to avoid paying you in all sorts of ways, including ways that are illegal.
We need single payer healthcare, medicare for all. If we all have healthcare, think of how many small businesses would start up. And why don’t we have single payer healthcare? I think the big corporations don’t want it.
Who is the man in the photograph? I don’t know. This is an old tintype. They came from my Great Aunt, Esther White Parr, married to Russel Parr. Perhaps they are Parrs, because my Uncle Rob did not know any of the people in the four tintypes I have. My sister and I used them for portraits in our china doll houses.I hope he is not the CEO of an insurance corporation, but then, all the white collar white men tried to dress that way then.
Discover and re-discover Mexico’s cuisine, culture and history through the recipes, backyard stories and other interesting findings of an expatriate in Canada
Engaging in some lyrical athletics whilst painting pictures with words and pounding the pavement. I run; blog; write poetry; chase after my kids & drink coffee.
Refugees welcome - Flüchtlinge willkommen I am teaching German to refugees. Ich unterrichte geflüchtete Menschen in der deutschen Sprache. I am writing this blog in English and German because my friends speak English and German. Ich schreibe auf Deutsch und Englisch, weil meine Freunde Deutsch und Englisch sprechen.










You must be logged in to post a comment.