The CDC has guidelines for Long Covid and it can qualify for disability in the United States.
Here: https://www.cdc.gov/coronavirus/2019-ncov/long-term-effects/index.html
And here: “As of July 2021, “long COVID,” also known as post-COVID conditions, can be considered a disability under the Americans with Disabilities Act (ADA). Learn more: Guidance on “Long COVID” as a Disability Under the ADA, Section“
Here is the list of “most common” symptoms from the CDC:
General symptoms
- Tiredness or fatigue that interferes with daily life
- Symptoms that get worse after physical or mental effort (also known as “post-exertional malaise”)
- Fever
Respiratory and heart symptoms
- Difficulty breathing or shortness of breath
- Cough
- Chest pain
- Fast-beating or pounding heart (also known as heart palpitations)
Neurological symptoms
- Difficulty thinking or concentrating (sometimes referred to as “brain fog”)
- Headache
- Sleep problems
- Dizziness when you stand up (lightheadedness)
- Pins-and-needles feelings
- Change in smell or taste
- Depression or anxiety
Digestive symptoms
Other symptoms
- Joint or muscle pain
- Rash
- Changes in menstrual cycles
There are recommendations for a work up by physicians. Depending on symptoms, this may include labs, ECG, echocardiogram (heart ultrasound), CT scan and other tests.
A friend has just gone through those four tests . They are “normal” except for her heart rate. At rest her heart rate is 70 with a normal oxygen level. Walking, her heart rate jumps to 135. Over 100 is abnormal in this athlete who is NOT exerting heavily.
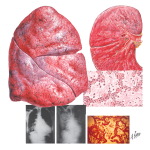
So WHAT is going on with NORMAL testing? I think this is “Covid-19 Viral Pneumonia”, a complication of Covid-19, just as “Influenza Viral Pneumonia” is a complication of influenza. Ralph Netter MD has an illustration of lungs from a person who died of influenza viral pneumonia: the lungs are swollen and inflamed and bruised. WHY is the testing “normal” then? The swelling is throughout the lungs, so a chest x-ray sees it as all the same density and a CT scan also sees it as all the same density. The lungs may have mildly decreased breath sounds, but the sounds are even throughout the lungs. The useful TEST is a walk test. I have tested patients with “walking pneumonia” in clinic for years: get a resting heart rate and oxygen level. Then have my patient walk up and down the hall three times and sit back down. Watch the heart rate and oxygen level. If the heart rate jumps 30 beats up or is over 100, the person needs to continue rest until the heart rate stays under 100 or jumps less than 30 beats. It is important to observe the heart rate until they recover. Sometimes the oxygen saturation will drop as the heart rate comes down, and some people qualify for oxygen. Steroids do not seem to work for this. The length of time to healing is not totally surprising, because a lobar pneumonia that is visible on chest xray takes 6-8 weeks to fully clear. It is not too amazing that a bad walking pneumonia could also take 6 weeks or more to clear. If the person returns to work too soon, they prolong the lung inflammation and they are at risk for exhaustion and for a secondary pneumonia. The treatment is REST REST REST and support.
Do they need oxygen? Currently oxygen is covered only if the person’s oxygen saturation drops down to 88%. However, I think that oxygen would help recovery and make them less exhausted. With my first walking pneumonia, which was influenza, my walking heart rate was 135 and my resting heart rate was 100. Both were abnormal for me. Neither I nor my physician could figure it out. This was in 2003. I did look in my Netter book: I took one look at the painting of the influenza lungs and shut the book. “Oh.” I thought. “That’s why I can’t breathe.” The image is here, though I wish it were bigger.
It took two months for my heart rate to come down, the lung swelling to improve, and me to return to work. I read the text of Dr. Netter’s image a year later and then I read an entire book about the 1918-1919 influenza. Since then I have walked people who come in complaining of exhaustion after a “cold” or “bad cough”. Viruses can cause this and so can bacteria: mycoplasma pneumonia, chlamydia pneumonia, pneumococcal pneumonia, legionella and strep A. If the fever is gone, the infection has probably resolved, but it still can take days or weeks for the lung tissue to recover.
For Covid-19, I would add a third test: walking with weights. We test cardiac patients by asking if they can carry two bags of groceries up a flight of stairs. That is 3 Mets, a measure of the heart load. We need to measure the lung load as well. If the lung tissue is swollen, the amount of airspace is cut down and can be half normal. The heart attempts to take up the slack. The person may tolerate a heart rate of 135 for a while, but it is like running a marathon. If they are older or have heart disease, this can trigger a heart attack. I would walk the person carrying hand weights, and see the recovery.
Also, brain fog is unsurprising. If your oxygen level is borderline, it is darn hard to think. I write really strange songs when I am hypoxic. I get goofy and feel weird. The fast heart rate also feels like anxiety: I think that the body is trying to tell me to rest.
The definition of Long Covid is symptoms after 30 days. Please see your physician if you are still ill and continue to have symptoms.
Blessings.
Here is a recent article about T-cells and inflammation in the lungs of Covid-19 patients: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8460308/
and this: https://www.frontiersin.org/articles/10.3389/fimmu.2020.589380/full
















{kind=link}
You must be logged in to post a comment.