

My theme is happy things, though sometimes they are things where I am trying to find the perspective to love what is happening.
When my son was little, I had Dr. Suess’s ABCs memorized: Ear, egg, elephant, E, e, e!
My words today are everybody, embody and evening.
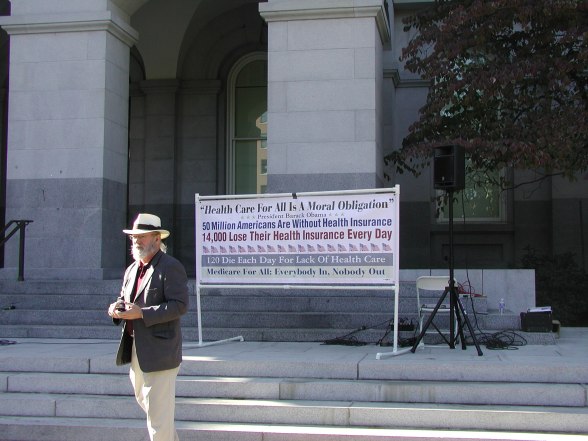
E for Everybody. Everybody in, nobody out! This is one of the calls for Healthcare for all, and I am still a Mad as Hell Doctor, working for single payer.
Our state representative was here a year ago and said that there is not a mandate for healthcare for all. I said, “I politely disagree. We already have a law in place that emergency rooms cannot turn anyone away. They cannot refuse to treat a person. This is a mandate for care. Unfortunately, the emergency room is the most expensive and inefficient care, unless you are about to die. The emergency room cannot do chronic care: it cannot help people stop smoking, help lower blood pressure, help people with chronic illness such as diabetes, do preventative care like pap smears and checking kidney function to stave off renal failure. We have the mandate: now we need the political will to change to a single payer system that gives good care. A patient can see me in my family practice clinic a dozen times for the cost of one emergency room visit.” S o, everybody in, nobody out. The law that insurance companies can ONLY keep 20 cents of every dollar does not comfort me: I want my dollar to go to health care for everyone and not 1/5 to profit!
Embody: what do I embody? What do you embody? Do you treat your body well? Do you thank it? What is it carrying?
I see people so fixed on success and progress and getting goals, that sometimes we don’t pay any attention to our bodies. We treat the body like a tool, like a hammer or a wrench, use and abuse it, try to make it conform to some idea of external beauty, get angry when it breaks down. Fix me back to where I was three years ago, when I could work 12 hours a day and never ever paid attention to my body. Bad food, tobacco, alcohol, marijuana, gallons of caffeine, energy drinks, sugar, illegal drugs, no exercise… and then we are surprised when it breaks down? Even exercise is seen as an inconvenient and necessary job, like buying new tires for the car. When people say get me back to where I was, I ask, “Back to working the 12 hours a day that caused this damage? Do you think that is a good idea?
And I include myself in that! I have had pneumonia with sepsis symptoms twice. The second time I thought, how dumb I am! My father died and I did not take any time off. I just kept working and added executor to my jobs and cried daily. Is it any surprise that after a year of that I became ill? Now my goal is to not do medicine for more than forty hours a week and to listen to my body and to take breaks!
Evening: the sunset. I am so grateful for the day, for the night, for the light changing and the world turning, for the stars and the moon and the sun and the glorious, gorgeous, generous world.
This is an evening photograph from Mauna Loa last week.









You must be logged in to post a comment.