Beloved
I don’t think I can bear this
It’s a good plan
To work five more years
And retire in better financial shape
House paid off
But it hurts so
My tattered bruised and battered heart
Already patched so many times
And to see so many people each day
Hurting
Why, Beloved?
Why don’t we mature?
Maybe I’ll be a tree again
Living wood
That bends and moves with the wind
That eats the sunlight
Drinks the rain
Endures the snow and drinks it as it melts
Until spring comes
And I stir and start to bud
Deciding when it’s time
To uncurl leaves in warm sun
_______________________
For the Ragtag Daily Prompt illusion. Or should it be delusion? Or survival? Or beyond that to peace?
I am working at a site in the greater Seattle area, but I am not going to say where. Why? Two reasons. One is that the patient diversity is huge: the organization is organized to take care of low income, uninsured and immigrant patients. The second is that I am still trying to decide if the balance of the organization is working. It may be working but it might not be working for me.
I am at a large clinic, with primary care, dental, behavioral health, a nutritionist, a pharmacy and three in person translators. In any one day I will probably use translators for at least six languages. English, Spanish, Dari, Hindi, Punjabi, Arabic, French, Somali and sometimes languages that I have to look up the country because I don’t know where that language is spoken. The work is fast and furious.
The overall no show rate is 20%. This makes the day very unpredictable. It can be very very fast and busy with everyone showing up and then later there are three no shows in a row. I think that the no show rate has been less than 20% but on Tuesday it was more. However, everyone showed up in the morning and there was a hospital follow up that should have had 40 minutes and only had 20 and of course then we ran later. My lunch theoretically starts at 12 but I went to lunch at 12:50 and came back 6 minutes late, at 1:06. Then people no showed while I worked to finish off everything from the morning. It did feel a bit nuts.
We are using the electronic medical record EPIC. I find EPIC epically frustrating. It is “feature rich” which means it has too many ways to do things. If I ask someone how to record a phone call to a patient, it takes eight steps. A week later I have to do it again, I ask again, and the next person shows me a DIFFERENT set of eight steps. And there have to be at least eight ways to do anything, so it is very confusing. Also, the “home” page can be personalized to the extent that people look at my version (I have not personalized it much) and say, “Mine looks different. I don’t know how to do that on yours.”
Whew. So, how to cope with the fast furious unpredictable schedule? I am “precharting”. For this Tuesday, I spent 70 minutes going through the patient charts on Saturday. Then I may know why they are coming in, if they had a heart attack two weeks ago and are following up, if it is a well child check and the last one was two years ago, if there are outstanding issues like a elevated liver tests or they have not been in for their out of control diabetes for a year. Then, of course, some of them do not show up. It is so busy that all I feel when someone no shows is some relief, like a ray of sunlight in a dark forest. Ok, the person who was horribly sick and in the hospital for a week and had surgery, they really do need to follow up. But I cannot make them, no one can.
We have live translators, outside translators who come with the patient, family sometimes translates and two phone translation systems. Our live translators cover the following. One Spanish only, one Dari, Arabic and ?maybe Russian. A third language. The third does Hindi, Punjabi and something else. I can’t tell by language who is a recent immigrant or refugee or who is a citizen of the United States for thirty years.
The clinic system has high standards for care of an often vulnerable population. However, I have not decided if it falls into a statement by my grandfather: “The higher the ideals of an organization, the worse its’ human relations.” My job in Alamosa had very high ideals, but I was fifth senior doctor out of 15 in a mere two years. A burnout job. This one has three new doctors coming in soon. My training and assistance to learn EPIC has been sparse and not up to my standards. If the new doctors are treated the same way then this is a burnout job as well. This is a place that I could work in intermittently alternating with other places in the country, but only if it is balanced for both the patients and the physicians. The jury is still out, but there are many red flags. It is a six month job and I am two months in, so we shall see.
The photograph is from Larrabee State Park this weekend. My daughter came out and saw many of her friends, stayed with me, and we camped for one night at Larrabee.
Should we worry about bird flu? Oh, yes, I think so. I have been wondering why we still have chicken to eat and chicken in the stores, if millions of chickens are being wiped out to try to prevent H5N1 bird influenza from moving into humans. This article explains in unreassuring detail how factory farms, packing chickens together, and killing them at 6 weeks old for meat, puts pressure on the virus to become more deadly and kill the host. In wild birds the influenza virus wants to spread, so it’s better not to kill the host fast. That is not true on our national and international big factory farms.
Firing the people working the track the H5N1 bird influenza and trying to stop it if it starts going human to human, well. Is that injustice or arrogance or stupidity? Or all three? And who wants to work for the government now? It is being treated as a corporation, but it isn’t a corporation. Public service often pays less. Good luck hiring the best and brightest who want to serve our country and humanity.
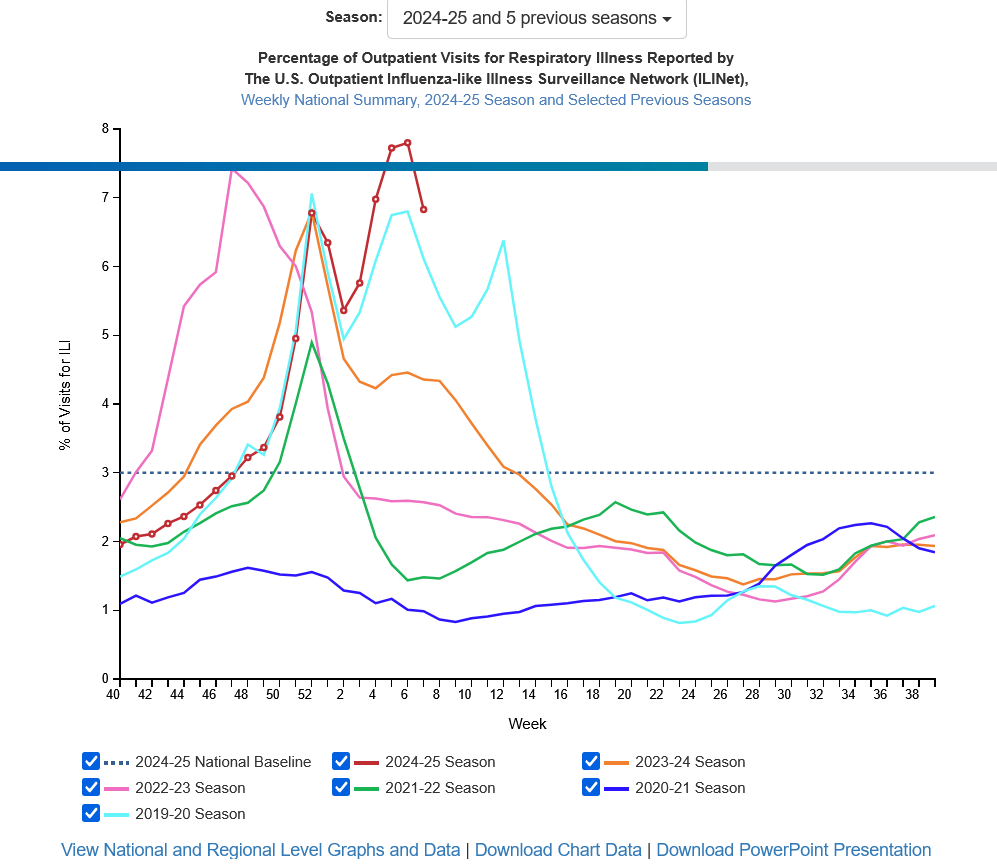
This is the worst year in the US for influenza since 2017-2018 so far. That is without the H5N1 bird influenza really getting in to people. Here is the graph for the week ending February 15th from the CDC. I keep an eye on it all through influenza season.
The article on H5N1 bird influenza is the best argument I’ve ever read for choosing not to eat meat. I like meat, but the factory farming is going to more countries. It may produce more eggs and more chickens, but if it is also the perfect breeding ground for lethal influenza, that changes my viewpoint. We cannot go on. We will have another pandemic.
I am writing daily, just not for the Ragtag Daily Prompt. Here is my short note today:
Dear President Trump: I strongly disagree with withdrawing the United States from the World Health Organization. One function of that organization is travel clinics. If a person is traveling to another country, they can find out what illnesses are present there and get immunizations and advice to avoid getting ill. This also helps physicians treat people who have returned from another country. The physician can contact a state health department which is in turn connected to the World Health Organization. This is a foolish, dramatic and unscientific decision on your part. I suggest that you reverse it immediately or resign as President.
________________
The question I have, is he closing the borders to United States citizens too? Without the travel clinics, who get information about each country from the World Health Organization, aren’t even our own state department employees at higher risk for illness? My son was an exchange student to southern Thailand. At the time he went, there was Japanese encephalitis. He was there two years after the tsunami. He got vaccinated for Japanese encephalitis before he went and he also took medicine to avoid malaria. So, are we not going to send or accept any more exchange students?
I strongly disagree with the decision to leave the World Health Organization and our country is on the verge of crazy.
I get a call from the hospital (this is over a year ago). They say, “Your friend is ready for discharge. What time can you pick her up?”
I reply, “Can she walk?”
“What?”
“She has three steps up into her house. Can she walk, because otherwise I can’t get her into her home.”
“Oh, uh, we will check.”
They call me back. “She can’t walk. She’ll have to stay another day.”
I knew that she couldn’t walk before they called. She could barely walk before the surgery and after anesthesia, surgery and a night in the hospital, her walking was worse. She had been falling 1-5 times at home and the surgeon knew that. He did not take it into account. The staff would have delivered her to my car in a wheelchair and then it would have been my problem.
She was confused by that afternoon, which is not uncommon in older people after anesthesia. She stayed in the hospital for six days and then went to rehab, because she still couldn’t walk safely.
Recently I have a patient, an elder, that I send to the emergency room for possible admission. He is admitted and discharged after two and a half days. Unfortunately he can barely walk and his wife is sick as well. The medicare rules say that he needs 72 hours in the hospital before he qualifies for rehab. We scramble in clinic to get them Home Health services, with a nurse check and physical therapy and occupational therapy, and I ask for Meals on Wheels. It turns out that Meals on Wheels will be able to deliver in two months.
The wife refuses to go to the emergency room. I tell her that if she does get sicker, that they both need to check in. The husband can barely walk and is not safe home alone. If one gets hospitalized, they both need it.
If you have a frail elder, be careful when you are called about discharge. Go look at them yourself, make sure that you see that they can get out of bed, get to the bathroom, walk up and down the hall. Can they eat? Do you have steps into your house or theirs and can they go up the steps? I got away with saying please check that my friend could walk because I am a physician, because I knew she couldn’t and because there was no one else to pick her up. Do NOT ask your elder. They may want nothing more than to go home and they may well exaggerate what they can do or be firmly in denial. You want them to be safe at home, to not fall, to not break a hip and to not be bedridden.
For an already frail elder, even two and a half days in bed contributes to weakness. And being sick makes them weaker. If they are barely walking when they are admitted, it may be worse even after just 2-3 days. I used to write for physical therapy evaluation and exercise when elder patients were admitted, to help them for discharge. Once I got a polite query from physical therapy saying, “This patient is on a ventilator. Do you still want a consult?” I reply, “Yes, please do passive range of motion, thank you!”
Your elder does not have to be doing rumbustious dancing before they go home, but they need to be able to manage stairs, manage the bathroom, manage walking so that they can get stronger. Otherwise a stay in a nursing home or rehabilitation facility may be much safer for everyone.
Yesterday was my second day in the third clinic in this system and the day went a bit sideways. I am in seeing a person with their spouse. We are all masked because this is a sick visit. I try to wear a mask for all the visits but occasionally take it off if someone really can’t hear me. I go to wash my hands. The sink is small and turns on by a motion sensor. It is supposed to turn itself off. It goes on but then will not turn off and is loud. I send a quick message to the clinic director after flailing at it a bit. Why a message? The cabinet under the sink is locked, so I can’t turn the water off. With my patient slightly deaf and masks and loud water, I finish the visit trying to yell things. Ridiculous and embarrassing but funny. The patient and spouse are older and know that things break. They are not upset. The clinic director arrives, has her try at flailing at the sensor, unlocks the cabinet and turns the water off.
I shake hands with my patient and they and their spouse leave. We are in room three. I go in room 4 to wash my hands, since my patient was blowing their nose, and guess what? Yes, the water turns on and won’t turn off. I get the clinic manager. “I broke the second sink. How about I go home now?”
She laughs. “I will put in a ticket for maintenance.” She unlocks the room 4 sink and turns it off. Now we have two rooms out of commission!
I am covering for Dr. X. “See, this just shows that I wash my hands and Dr. X didn’t.” Not really. Dr. X has been out for a month already.
“Maybe it’s because they haven’t been used in a month,” says the medical assistant. We shut down those two rooms and I go into room 2 with some trepidation. The sink does not break.
Maintenance show up early afternoon and replaces the sink sensor batteries in room 3 and 4. They work just fine after that. It turns out that there are two other sinks not working, but there are patient visits going on, so maintenance will come back. The alcohol hand sanitizer makes my hands itch, so I prefer soap and water.
Isn’t technology great? Except when it breaks. I felt silly and helpless, since I was in a brand new place and the cabinets were locked!
I admonish all the doctors, do wash your hands! Even if the sink batteries need to be replaced more often.
I was out of clinic for two years and then very part time for a year and now not quite full time as a temp. I bargained to not quite be full time.
The electronic medical record is having a consequence, along with the pressure to see more people faster. The primary care doctors, at least the younger ones, do not seem to call their peer specialists any more. (Family Medicine is a specialty, just as Internal Medicine and Obstetrics/Gynecology are.) I called a gastroenterologist and left a message last week about a difficult and complex patient. The patient had cried three times during our visit. The gastroenterologist was very pleased I had called, was helpful, agreed with my plan of using the side effects of an antidepressant to try to help our patient, and thanked me three times for calling her. Wow. I am used to calling because during my first decade in Washington State, our rural hospital had Family Practice, General Surgery, a Urologist, Orthopedics and a Neurologist. For anything else, we called. I knew specialists on the phone for a one hundred mile radius and some knew me well enough that they’d say a cheery hi.
Now communication is by electronic medical record and email on the medical record and by (HORRORS) TEXT. Ugh. I think that there is quite a lot of handing the patient off by referring them to the Rheumatologist or Cardiologist or whatever, but the local Rheumatologist is booked out until February for new patients. That leaves the patient in a sort of despair if we don’t keep checking in on the problem. If I am worried, I call the Rheumatologist and say, “What can I do now?” I’ve had two people dropping into kidney failure and both times a call to the Nephrologist was very very helpful. I ordered the next tests that they wanted and got things rolling. One patient just got the renal ultrasound about three months after it was ordered. Sigh.
I have one patient who is booked in February for a specialist. I called that specialist too, they did not want any further tests. I told the patient, “You aren’t that sick so you won’t be seen for a while. It isn’t first come first serve: it is sickest first. We all have to save room for the emergencies and sometimes those are overwhelming.” The specialist agreed and the patient is fine with that and I think pleased to know that we do not think she’s that sick. She feels better. If things get worse, she is to come see me and might get moved up. Neither I nor the specialist think that will happen.
Is this conservation of energy, to communicate by email and text? I don’t think so. I think sometimes a phone call is much more helpful, because the other physician knows exactly what I am worrying about and they can tell me their thoughts swiftly. Sometimes they want me to start or change a medicine. Things can get lost in the overwhelming piles of data and the emails and labs and xrays and specialist notes all flowing in.
My Uncle Jim (known as AHU for Ancient Honorable Uncle Jim) used to sing part of this:
Yeah, that’s just how I call my fellow specialists.
For the Ragtag Daily Prompt: conservation. Don’t cats win at conservation of energy?
I ran my own small clinic from 2010 to 2022, working somewhere else, got Covid, was on oxygen for a year and a half, did some healing and then came back to work.
There has been a culture change in medicine that feels very strange to me. I did not notice it because I was in a solo clinic and not “part of the system”.
All the doctors, providers, are more isolated. I got a compliment yesterday when I was doing a “warm hand off” of the most sick or complicated patients, three new diabetics, a person with cancer, a person with a genetic heart problem. The doctor who I was handing off to is in the same clinic but we have barely talked since May. I don’t know her at all. She complimented me on excellent care “and calling specialists”.
I thought, huh. But I think that is a dinosaur doctor thing. I think mostly people communicate through the electronic medical record email, send messages about patients. For the decade that I was solo, I had to call other specialists because I was on a different electronic medical record. The email didn’t connect. The hospital reluctantly gave me a “link” to their system, but it was only a link to look. I could not write or send anything.
About two months ago I got an echocardiogram result. I read it and thought, ok, it’s not normal but what does it mean? Outflow obstruction by the thickened heart wall. Hmm. I called cardiology and spoke to the cardiologist who read it. He sounded surprised and said, “Idiopathic hypertrophic cardiomyopathy, most likely. It’s a classic echo.” “So, what do I do?” “Send him to me.” “Anything that I should change meanwhile?” “Yes,” says the cardiologist. He had me stop one medicine and start another. “No vasodilators and the beta blocker slowing the heart rate should help decrease the outflow obstruction.” “Got it.” I said. He also gave me two more tests to order.
I referred the patient to cardiology but it was a month before he got in. The two tests were done and they ordered more. If the diagnosis is correct, he’ll be sent to a special clinic in Denver. I called my patient while we were waiting for the cardiology visit. The medicine change had not made much difference as far as he could tell.
I was also told when I got here that I would never get a local nephrologist to see a patient, they were two busy. However, I have called two nephrologists about two patients and both took the patient and again, gave me instructions.
Two specialties have been very difficult to contact: orthopedics and gastroenterology. I have no idea why they are so difficult.
I can see that email feels faster. But there is no human contact, asking follow up questions is difficult, I don’t get that bit of further helpful education: this is what you do next. I have learned so much over the years by touching base with specialists. Once I fussed at a patient to go to hematology oncology about their high platelet count. The patient didn’t want to. He came back and said, “Apparently I have this newly found genetic problem. They put me on two medicines, not expensive. And I feel better than I have in 20 years.” I asked the oncologist about it the next time I called. He lit up, excited, and told me about the JAK-2 mutation. It is so exciting to learn about new areas in medicine and my patient says, “I have to thank you for pushing me to see the oncologist. I feel so much better.” Wow and cool.
Clinic feels like I am mostly isolated, a silo, an island, rarely talk to the other physicians unless I go to find them. I think hospital administrations like this, keeping the physicians in line by having their schedule be so packed that they almost never talk to each other. What a good way to keep physicians from interfering in the money making production! Ugh, I think it is quite horrible and unhealthy for the providers and for our countries medical system in the long run. I was seriously less lonely in a solo clinic.
The prognosis for our current medical system is very poor. The patients say to me, “Why do my doctors keep leaving?” They aren’t attached, they are isolated, I don’t think the physicians know what they are missing. Colleagues. Not silos.
Honey is older, nearly thirty years since that first feeling of being bitten by ants. She is back in corporate medicine, as a temp. Temporary, short term, maybe that will work better.
It is a joy to go in a room and be alone with a person and their monsters. Theirs and hers. Sometimes the younger ones haven’t experienced it, they are terrified if one of their monsters becomes a little bit visible, they hate seeing them. Honey tries to be gentle. If they only want to talk about the sore shoulder and not the stress and violence, well, she leaves the door open a crack. Sometimes the monsters cry.
Older people may be stiff to start with, but when they realize their monsters are seen, acknowledged, this isn’t another robot doctor in to say increase your diabetes medicine, lower your diabetes medicine, tell them a plan without ever connecting, the older ones lean back, sigh, and relax. The monsters play on the floor, Honey’s monsters playing with theirs, happy, engaged.
The hard part is the clinic staff. Honey is with them daily. The medical assistants are young. They kick their monsters aside as they walk down the hall. It is terribly hard and heartbreaking to work at her desk, with the medical assistants’ monsters cowering under their desks, kicked, abused, silent tears and holding bruises. Honey’s monsters mind. They climb into her lap and hide their faces in her shirt, under her jacket, peer over her shoulder. They don’t understand! Why can’t she be nice to THESE monsters?
Honey whispers to her monsters when the medical assistants are rooming patients. “I am so sorry, loves. If I acknowledge these, the monsters of the women working, I become a demon. It is very hard to share an office, no wonder I worked in a clinic alone for eleven years.” Honey has been through that. It is still inconceivable that some people don’t see the monsters at all. Is it learned blindness? Or just not developed unless someone had to learn it? Unless someone grows up in terror and seeing the monsters is the only way to survive.
Honey thinks some people learn to see them as adults, at least their own monsters. Hard enough to do that, without seeing the monsters clinging to other people.
Honey is tired of her monsters crying in sympathy with the staff’s monsters. She thinks maybe there are small crumbs that she can leave for these demons. Little gifts. Her monsters can creep under the desk when she is the only one in the room and leave something. A flower. A dust bunny. A crumb of a crisp. A small rock. A little gift to let them know they are seen and loved. A poem. A prayer. Just a tiny bit of love.
On Friday in the morning I took notes on paper. I was attending a conference on diabetes on Zoom. There are three new things added to the diabetes guidelines. It is now impossible to do a visit about diabetes and actually talk to the human being who has diabetes. We’ll be too busy doing the stupid checklists.
The personnel person stopped by. I said I was taking notes. “On PAPER? You are killing me!”
“Ok. I will use yarn this afternoon.” I drove home and got my knitting and worked on a sock in the afternoon. All the clinics were having a slow day. I guess the kids are getting out of school and everyone is feeling good. Or panicked.
I retain as much information knitting as I do taking notes. Tactile-auditory learner and the controlled fidgeting of knitting helps me stay awake, retain information, and produce socks and others items. I wear the socks more than I reread the notes.
I still like paper. I keep a paper journal. I wanted notes from the most complex lecture. The new medicines are jockeying for position but right now there are different indications for each one, so it’s rather confusing. They said that Type II Diabetes takes two hours daily to manage “correctly”. And that Type I and Type II on insulin take 3 or more. We are supposed to check for Diabetes Distress, which is not depression, exactly. I think I need to be checked for Guideline Distress and Contact Diabetes Distress, sigh. At least the Diabetes Distress speaker thought we should talk to the patient, though I think the talking should have been long before that. Medicine in the US is a mess.
I used the back of the clinic schedules for notes. I do print it out daily. It’s to try to run on time. What time am I supposed to see the patient, but they can be up to 7 minutes late and then the medical assistant still has to “room” them (yes, room has been verbed). Then I can go see them. So the theoretical starting time and the actual starting time can vary quite a bit. I don’t feel bad about being twenty minutes late if I didn’t get to go in the room with the last patient until twenty minutes late. Maybe a no show will let me catch up. Or not.
Discover and re-discover Mexico’s cuisine, culture and history through the recipes, backyard stories and other interesting findings of an expatriate in Canada
Engaging in some lyrical athletics whilst painting pictures with words and pounding the pavement. I run; blog; write poetry; chase after my kids & drink coffee.
Refugees welcome - Flüchtlinge willkommen I am teaching German to refugees. Ich unterrichte geflüchtete Menschen in der deutschen Sprache. I am writing this blog in English and German because my friends speak English and German. Ich schreibe auf Deutsch und Englisch, weil meine Freunde Deutsch und Englisch sprechen.












You must be logged in to post a comment.